
Cholesterol isn’t the problem
Eating cholesterol is not bad. And neither is most fat really (the saturated kind included).
Anyone about to stop reading and write this off as nonsense, here is some science:
- The cholesterol hypothesis was based on flawed epidemiological studies (Ancel Keys1)
- and then propagated by political dramaticism (George McGovern2).
- Evidence to the contrary was dismissed in multiple cases 3–5.
- By now highly acclaimed instituted have stated cholesterol and saturated fats are not very relevant for heart disease.
- This includes the WHO6 and the Cochrane Collaboration7. Cholesterol recommendations now are mostly based on convention, not science. My goal here is to sum cholesterol research up for you.
But, but why?!
Good question. And one with a good answer. The easiest way to explain what happened is to look at how the cholesterol theory was formed. We’ll run through the history briefly. You’ll easily be able to see how we got to where we are now.
Pre 1970
Mostly epidemiological studies. This is like, “The Spanish have darker skin than the Dutch. Spain has more sun that the Netherlands. The sun probably makes your skin darker”. They are only indications though, because you could also do an epidemiological study that finds “People in the Netherlands are white and eat cheese. People in South Africa are black and rarely eat cheese. Cheese probably makes you go white”.
- 1951: Ancel Keys compares countries with high and low cholesterol intake, and finds those with high cholesterol intake have higher incidence of heart disease8
- 1955: Eisenhower has a heart attack, making this a hot topic9
- 1957: Keys compares countries with high and low fat intake, and finds those with high intake have more heart disease10
- 1961: Times magazine publishes Keys stating we should consume max 15% of our diets in fats11,12
- 60’s: Big studies found no clear link between cholesterol and heart disease3–5,13
- 1970: Keys publishes a study drawing weak conclusions in favor of the hypothesis14. He himself spoke in terms of “tendency of incidence”
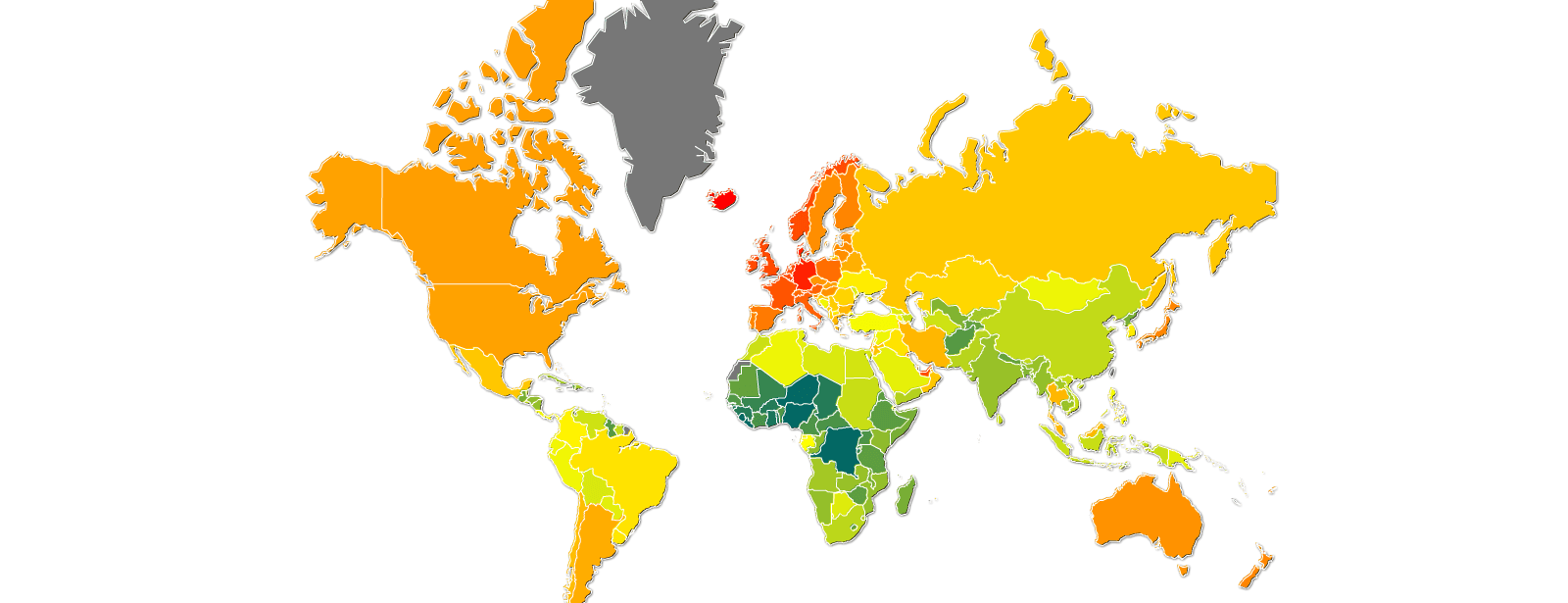
Cholesterol intake map15
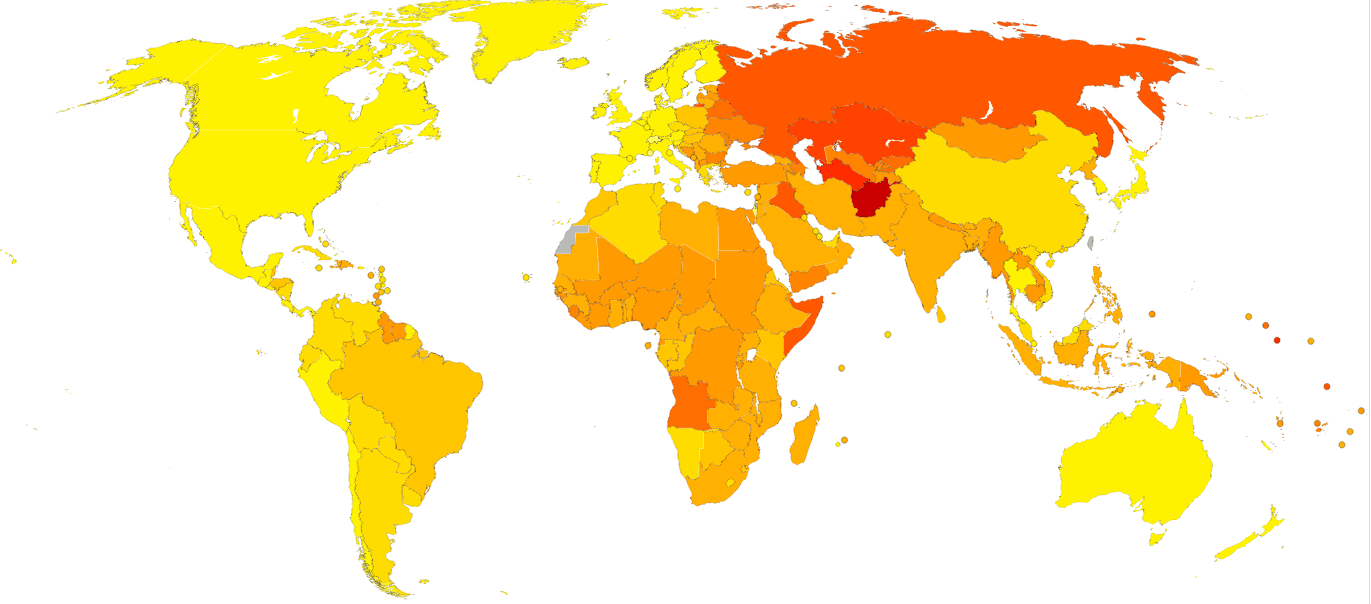
Age-standardized disability-adjusted life year (DALY) rates from Cardiovascular diseases by country16
After 1973
Clinical trials start. Thank god, finally real science.
- 1973: Big clinical study don, let’s look at their conclusion: _“For the entire study population, no differences between the treatment and control groups were observed for cardiovascular events, cardiovascular deaths, or total mortality.”17 This only published in 1989 because the researchers were disappointed in the results.
- 1977: Dietary recommendations were made stating cholesterol and fat intake should be reduced18. The committee reportedly said “we don’t have the luxury of time to find the truth before making policy”
- 1977: We (humans) learn the difference between HDL and LDL cholesterol, and find high LDL predicts heart disease19,20
- 1981: Huge study finds higher saturated fat increases life span and decreases heart disease. Low HDL predicted heart disease 4x better than high LDL21.
- 1981: A research group digs into old studies and finds that the conclusions made about fat and cholesterol have no basis in their data22. The media (Washington post23, NY Times23) somehow concluded that this means we should decrease fat and cholesterol intake (?!).
- 1990: The American Heart Association and National Heart, Lung, and Blood Institute state the 1981 study shows impressive results and clear correlations24. (Whatever these people smoke, don’t touch it)
Early 80’s: $265,000,000 worth of disappointment
- 1982: MRFIT study. 17.9 deaths per 1,000 in the intervention group and 19.3 per 1,000 in the control group. Total mortality rates were 41.2 per 1,000 (intervention) and 40.4 per 1,000 (control)25. Conclusion: no statistical significance
- 1984: LRC-CPPT study26. Found lower deaths when using a cholesterol lowering drug. Rightfully they stated that LRCPPT was not designed to assess whether lowering cholesterol by diet prevents Coronary Heart Disease. Why? Because saying a drug decreases heart disease because it lowers cholesterol is like saying aspirin reduces heart disease because it cures headaches.
- 1984: Times smells sensational drama and publishes “Sorry, it’s true. Cholesterol is a killer”.27–29
- 1985: The NIH holds a consensus conference and conclude “There is no doubt that a low-fat diet will afford significant protection against coronary heart disease to every American over the age of two”30. One of the co-authors noted “If there had been a consensus you wouldn’t have had to have a consensus conference.”
- 1989: Organizations like the National Academy of Sciences blindly follow the “consensus”31.
Around 2000, heart disease on the rise, science gets suspicious
- 1999: The prestigious Cochrane Collaboration does a meta-analysis. Their most recent version states: _“There were no clear effects of dietary fat changes on total mortality or cardiovascular mortality.” 7
- 2006: The Cochrane Collaboration analyses if the usual interventions (low cholesterol etc) work. They find it does not help in the general population32.
- 2006: Women's Health Initiative Randomized Controlled Dietary Modification Trial33. Reduced fat intake did not significantly reduce the risk of CHD, stroke, or CVD in postmenopausal women and achieved only modest effects on CVD risk factors
21st century: comparing diets
- 2003: slightly larger amount of weight loss in a low carb diet than in a high carb diet group, the results became insignificant after 1 year. HDL levels were significantly increased (that’s good). Triglycerides were significantly reduced (that’s good).34
- 2007: Low carb vs low fat. Low carb wins with: Biggest weight reduction over 12 months, drastic decrease in triglycerides, drastic increase in HDL, largest decrease in diastolic blood pressure35
- 2008: Low carb vs low fat diets. Low carb wins again with: a significant increase in HDL, a significant decrease in triglycerides36
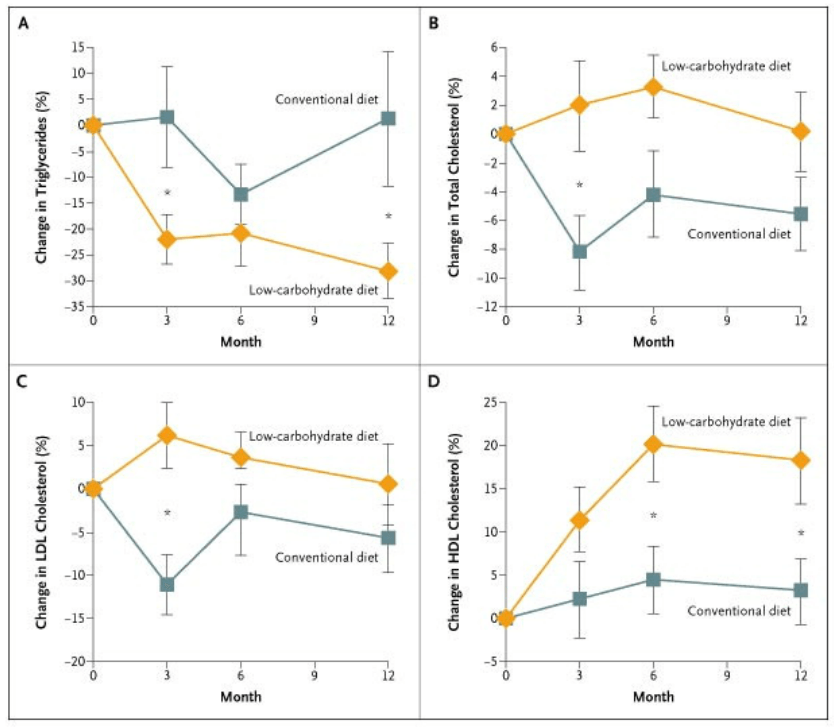 2003 study. Note especially A and D34
2003 study. Note especially A and D34
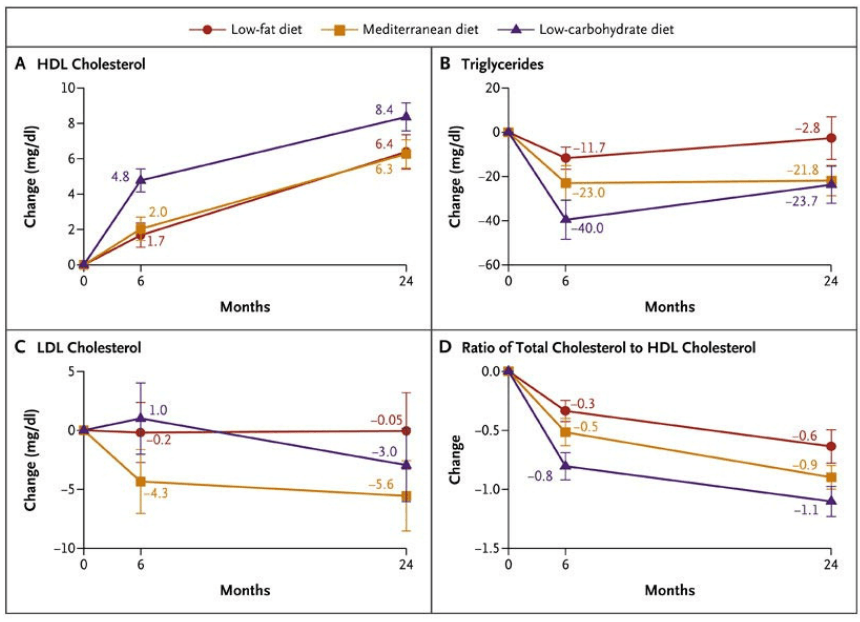
2008 study. Low carbohydrate beats low fat36 And voila, we arrive at the state of science in 2014 (ish). We now know that:
- Saturated fat and cholesterol intake are inreliable predictors for heart disease
- Cholesterol lowering medicine lowers heart disease. However making a link there is like saying aspirin prevents heart disease because it cures headaches
- Low fat diets do not improve cholesterol and triglyceride levels much, but low carb ones do
Some actual science for you
Enough with the history lesson. Ultimately human biology has to prove or disprove this kind of thing. So let’s have a look at our body then. First some facts:
- A typical dietary intake of cholesterol is 300 mg a day
- A typical human body produces 1000mg of cholesterol a day
What?! Yes. Doesn’t it seem a bit ineffective to target the 300mg of cholesterol you eat? Especially since your liver will probably just produce more to compensate? And this is not even new knowledge, it’s literally textbook science.
Cholesterol for 5 year olds
The cholesterol in an egg is not the cholesterol in your blood. The stuff in an egg is loose little molecules. The stuff in your body is complex balls made of cholesterol and proteins. You have a couple of types, the most discussed are:
- LDL (fluffy ball of cholesterol+proteins, considered bad)
- HDL (dense cholesterol+protein ball, considered good)
The most important thing to know about cholesterol is that your body can’t function without it. It is used to keep your cells stable, to produce hormones (hello testosterone and estrogen) and in digestion.
LDL vs HDL for 5 year olds
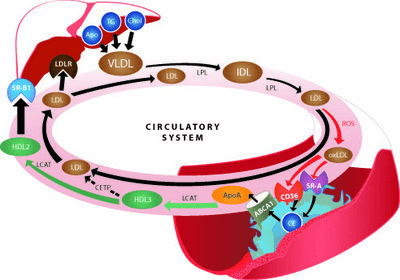
There are some nuances and complexities, but basically the story is like this:
- LDL is a fluffy cholesterol ball that carries cholesterol from the liver to the body
- HDL is a dense cholesterol ball that carries excess cholesterol from the body to the liver
As you can see it’s a bit more complex, but the gist of it is simple37
LDL and HDL levels are not very interesting on their own. What’s interesting is whether they are in balance. After all, if you carry a lot of cholesterol in LDL but the HDL brings the excess back, you’re not in trouble really.
The liver is central
In this whole process the liver is the spider in the proverbial web. If your cholesterol is too low it will sense this and distribute more. If you have too much, it will compensate for that. Let me repeat that: your liver is supposed to be able to balance high cholesterol in your blood. At low cholesterol levels SREBP sensors trigger more cholesterol creation38–40. At high cholesterol HMG-CoA sensors trigger compensation mechanisms41.
So what’s the issue then?
Short version: foods with a high glycemic index (GI) and fructose in particular. Long version: there isn’t really one. Plenty of studies have found the benefits of low carbohydrate34–36 and low GI42,43 lifestyles with regards to LDL, HDL and triglyceride levels. The liver can’t handle high quantities of fructose well. By the way, 50% of ‘regular’ sugar is fructose, don’t worry about fruit killing you.
Glycemic index for newbies
The GI is a measure of how big of a glucose and insulin spike a food/meal causes.
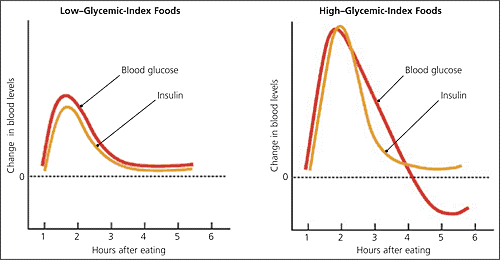
Low vs High GI foods44
You probably already know the scale a little, but just never thought about it:
- Worst: processed sugars (especially liquids, including fruit juice)
- Bad: Processed ‘white’ carbohydrates like flour, rice, pasta, bread etc
- No good: potatoes, starchy stuff. Especially in large quantities
- Ok: Generally vegetables, nuts, fats, protein
The problem is that people pay attention to the wrong things. Most people consider a hamburger bad because of fat. The fat doesn’t matter so much. The bun made of cardboard-like bread is. Same for fat/cholesterol rich steak. Doesn’t matter at all, so long as you don’t bulk up on white bread and cheap pasta while you eat it.
Get the full research
This can be quite overwhelming I know. This research took me quite a while, and on multiple occasions I looked up from my laptop and said “how is this even possible?”. If you want to view the full research file click here